ABSTRACT
- Hypoglycemia in people with type 2 diabetes mellitus (T2DM) is troublesome and an important barrier to diabetes management. Although more intensive glycemic control is emphasized to prevent diabetes-related long-term complications, it raises the risk of hypoglycemia in people with T2DM. Severe hypoglycemia (SH), defined as critical events characterized by altered mental and/or physical status requiring assistance for recovery, is considered an advanced and life-threatening form of hypoglycemia. The detection of SH is an important issue because it is associated with further adverse clinical outcomes such as cardiovascular events, mortality, cognitive impairment, and decreased quality of life. By identifying the potential risk factors for SH and introducing measures to minimize SH, SH itself and subsequent harmful clinical outcomes could be prevented in people with T2DM. The traditional risk factors for SH in T2DM, such as older age, long-standing diabetes with decreased insulin secretion, advanced vascular complications, serious comorbidities, and insulin use, are usually unmodifiable. However, unhealthy lifestyle factors, defined as current smoking, heavy alcohol consumption, and lack of regular exercise, can be improved through active patient education. In recent research, greater adherence to healthy lifestyle factors and any improvement in unhealthy lifestyle habits were found to be associated with a substantially lower risk of SH in individuals with T2DM. As well as being an essential component of diabetes self-care and optimal glycemic control, lifestyle modification probably contributes to the prevention of SH in individuals with T2DM.
-
Keywords: Type 2 diabetes mellitus; Severe hypoglycemia; Cardiovascular diseases; Lifestyle factors
INTRODUCTION
- Hypoglycemia, defined as a measured glucose level <70 mg/dL regardless of the severity of accompanying hypoglycemic symptoms, is considered clinically important for patients with diabetes [1,2]. An increase in hypoglycemia frequency or severity is a major barrier to optimal glycemic control and has a negative impact on health-related quality of life and the overall burden on healthcare resource use in both type 1 diabetes mellitus and type 2 diabetes mellitus (T2DM) [3,4]. Severe hypoglycemia (SH), classically defined as a hypoglycemic event requiring the assistance of another person, is of special concern for diabetes management [5,6]. Both recent and lifetime SH have been found to be associated with impaired cognition or dementia, impaired cognition or dementia, incident falls, irreversible brain damage, cardiovascular (CV) events, and fatal arrhythmia [7]. Therefore, diabetes treatment-related SH should be avoided, especially for elderly patients with diabetes.
- The American Diabetes Association and Endocrine Society workgroup on hypoglycemia adapted the three-level classification of iatrogenic hypoglycemia in diabetes proposed by the International Hypoglycemia Study Group (Table 1) [1,5–8]. In 2017, the International Hypoglycaemia Study Group also recommended that a blood glucose level <54 mg/dL is sufficiently low to indicate serious, clinically important hypoglycemia in patients with diabetes [5,8]. Notably, it proposed expanding the previous definition of SH as a hypoglycemic event requiring the assistance of another person in diabetes to include a measured glucose level <50 mg/dL, a level associated with cardiac arrhythmia and sudden death [5–9].
EPIDEMIOLOGY OF SH IN PATIENTS WITH TYPE 2 DIABETES IN KOREA
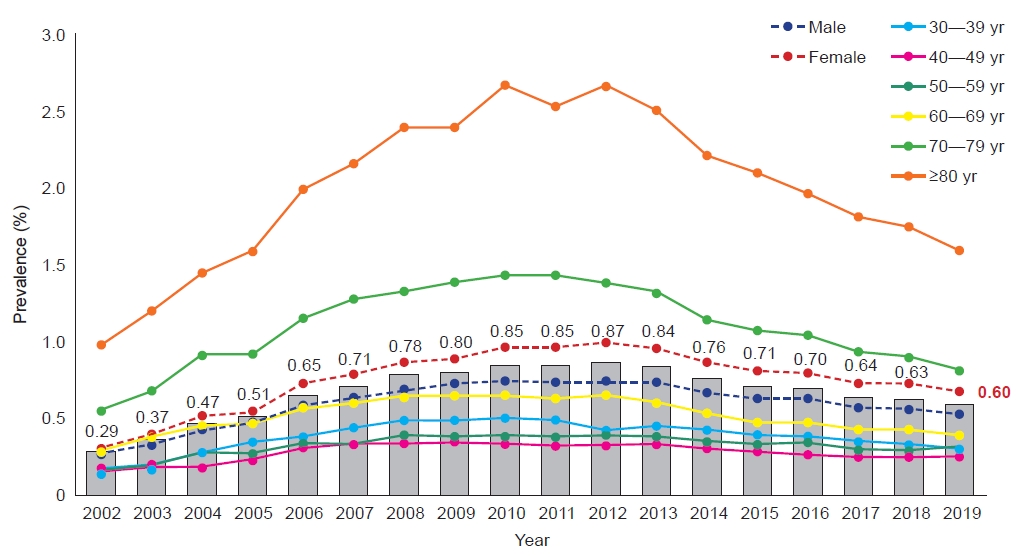
- We previously investigated the trends of SH in Korean patients with T2DM using the Korean National Health Insurance Service (NHIS) database. The prevalence of SH events in T2DM patients increased from 2002 to 2012; however, it decreased between 2012 and 2019 (Fig. 1) [10]. However, because the prevalence of T2DM has steadily increased, the absolute number of patients experiencing SH has actually increased during the past 17 years, despite several efforts to reduce SH [10,11]. Roughly 23,000 SH events occur in Korea every year, and the prevalence of SH was 0.6%, with an incidence rate of 4.43 per 1,000 person-years, in 2019 (Fig. 1) [10]. In particular, 15% to 17% of patients with SH experienced at least one previous episode of SH within the preceding 3 years.
- In general, hypoglycemia is caused by glucose-lowering medications such as insulin, a sulfonylurea, or a glinide. Therefore, the reduction in the incidence of SH seems to be related to the increased prescription rate of antihyperglycemic medications without hypoglycemia risk (dipeptidylpeptidase-4 inhibitors, glucagon-like peptide-1 receptor agonists [GLP-1RAs], or sodium-glucose cotransporter-2 [SGLT2] inhibitors), less strict hemoglobin A1c (HbA1c) goals, the individualization of diabetes treatment, and diabetes education for preventing hypoglycemia [12–14].
SH AND CV OUTCOMES IN T2DM
- The relationship between SH and CV disease (CVD) outcomes or mortality is supported by many previous studies [15–18]. Most of the available evidence from large epidemiological studies has shown a positive association between hypoglycemia (severe or nonsevere) and the risk of CVD events or death [19,20]. The results from the Trial Comparing Cardiovascular Safety of Insulin Degludec vs. Insulin Glargine in Patients With Type 2 Diabetes at High Risk of Cardiovascular Events (DEVOTE) population demonstrated an association between SH events and a higher risk of all-cause mortality, particularly in the short term after an SH episode [16]. According to a prospective cohort analysis of 1,209 participants with diagnosed diabetes from the Atherosclerosis Risk in Communities (ARIC) study, SH was a significant and potent marker of high risk for CV events and mortality [21]. A meta-analysis found that, in T2DM patients, the occurrence of an SH event was associated with about a twofold increase in the risk of all-cause mortality, CV mortality, and major adverse CV events [22]. We also investigated the association between SH and subsequent CVD and mortality events, and found an increased risk of myocardial infarction, stroke, heart failure, and all-cause mortality in Korean patients with T2DM who experienced an SH event with a dose-response, temporal relationship [23]. A consistent causal relationship between SH and CVD outcomes was found in Asian populations [23,24]. SH was also associated with the risk of hospitalization and mortality, mainly in elderly patients, and it may be predictive of future CV events in patients with diabetes who have pre-existing heart disease and obesity [25].
- Hypoglycemia has been shown to exert arrhythmogenic effects. Prior SH events were associated with a higher risk of new-onset atrial fibrillation (hazard ratio [HR], 1.10; 95% confidence interval [CI], 1.01–1.19) and all-cause mortality (HR, 1.57; 95% CI, 1.50–1.64) in Korean patients with T2DM [26]. The mean length of the corrected QT interval was also significantly prolonged in patients with diabetes presenting to the emergency department during or soon after an SH episode [27–29]. In a large cohort of adults with T2DM enrolled in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study, SH was independently associated with a 49% higher relative risk of heart failure (HR, 1.49; 95% CI, 1.01–2.21) [30].
PATHOGENESIS OF SH AND ITS EFFECTS ON CARDIAC FUNCTION
- Hypoglycemia is associated with several changes on electrocardiography, including ST-segment depression consistent with ischemia, heart rate variability, and QT prolongation that can be associated with arrhythmias and increased mortality [31–33]. The parasympathetic nervous system was identified as the primary mediator of SH-induced cardiac arrhythmias in a nondiabetic rodent model [34]. In addition, hypoglycemia was found to increase blood viscosity, platelet aggregation, plasminogen activator inhibitor-1, thromboglobulin, coagulation factor VIII, von Willebrand factor, and thrombin generation, resulting a hypercoagulable and atherothrombotic status [15,35–37]. In older adults, SH history was associated with alterations in cardiac function, including lower ejection fraction, greater left ventricular mass and chamber size, and impaired left ventricular filling [38].
- SH exacerbated myocardial injury and enhanced myocardial inflammation in diabetic mice. With enhanced production of myocardial proinflammatory cytokines and oxidative stress, myocardial metabolic remodeling was mediated by peroxisome proliferator-activated receptor beta or delta, leading to myocardial injury and dysfunction triggered by hypoglycemia in diabetic mice, but not in controls [39].
RISK FACTORS FOR SH IN T2DM
- Various studies have identified risk factors for SH in patients with T2DM. Older age, sulfonylureas and/or insulin treatment, intensive glycemic control, low HbA1c values, lower body mass index, longer duration of diabetes with insufficient insulin secretion, poor cognitive function, current use of various medications (polypharmacy in addition to antidiabetic drugs), a greater prevalence of coexisting multimorbidity (such as cancer, myocardial infarction, heart failure, peripheral arterial disease, atrial fibrillation, or stroke), renal dysfunction (low estimated glomerular filtration rate, proteinuria), a short life expectancy, severe vascular complications or severe comorbidities, and a prior history of SH significantly increase SH development [5,22,40–45]. The ARIC study showed that glucose fluctuations and the level of activities of daily living could be associated with the incidence of SH, as well as traditional risk factors [44]. Definite cardiovascular autonomic neuropathy was also an independent prognostic factor for the development of SH in patients with T2DM [40].
- Remarkably, in addition to the clinical characteristics and underlying comorbidities mentioned above, unhealthy lifestyle factors such as alcohol abuse or current smoking were associated with an increased risk of SH in patients with diabetes [46,47]. Real-world nested case-control data demonstrated that people with T2DM in poor health and with some lifestyle behaviors were more vulnerable to developing SH [46]. Alcohol can suppress hepatic gluconeogenesis, thereby interfering with the counter-regulatory response to hypoglycemia, and it diminishes awareness of hypoglycemia [48,49]. Smoking may reduce insulin clearance in people with T2DM, leading to hyperinsulinemia, an increased risk of postprandial hypoglycemia, and poorer overall metabolic control [50,51]. It is also important to note that alcohol abuse and smoking tend to be more prevalent in people with other behavioral risk factors, including poor diet, which can be associated with poor glycemic control [46,52]. These findings provide important clinical evidence regarding correctable and modifiable risk factors for the prevention of SH, especially in high-risk populations.
IS SH PREVENTABLE? A FOCUS ON LIFESTYLE MODIFICATION
- Considering the harmful clinical consequences of SH, more attention and proper strategies for SH are needed in patients at high risk for SH. Screening and stratifying high-risk patients for SH can be conducted using a risk prediction model, which may also be a useful tool for individualized care in routine clinical practice [15,41]. Recent trials have shown that the use of newer antidiabetic medications (GLP-1RAs and SGLT2 inhibitors) demonstrated advantages in reducing CV outcomes among individuals with T2DM and established CVD or those at high risk for CVD, without increasing the risk of SH [14,15,53–55]. Less glycemic target goals (i.e., higher HbA1c) with intensive individualized diabetes education are appropriate for those who have previously experienced SH or potentially are at high risk for SH [1,9,13,14]. Frequent glucose monitoring using a continuous glucose monitoring system has been useful for identifying undetected recurrent hypoglycemia and for safe titration of medications [1,14,56].
- Although many clinical risk factors have been recognized as risk factors for SH in T2DM, most of them are not modifiable or correctable. Therefore, the strategy for prevention of SH has mainly focused on education, glucose monitoring, or dose adjustment of antihyperglycemic agents [1,14,56].
- Interestingly, our recent study demonstrated that behavioral modification from an unhealthy to a healthier lifestyle was significantly associated with lower SH development among adults with T2DM. From health checkup self-report questionnaires using the Korean NHIS database, information was collected on patients’ history of smoking, alcohol consumption, and exercise habits. Unhealthy lifestyle factors were defined as follows: current smoking, heavy alcohol consumption (≥30 g/day), and a lack of regular exercise (moderate-intensity physical activity for <30 min/day, <5 times/wk or strenuous-intensity physical activity for <20 min/day, <3 times/wk) [47]. In this cohort study using the Korean NHIS database, current smoking, heavy alcohol consumption, and a lack of regular exercise were associated with 28%, 22%, and 21% higher risks for new-onset SH in patients with T2DM, respectively [47]. Combinations of these three unhealthy factors were significantly associated with a higher risk of incident SH in a dose-dependent manner. Individuals with all three unhealthy lifestyle factors showed an 81% higher risk of SH than those without any unhealthy lifestyle factors [47]. However, any improvement of unhealthy lifestyle factors, such as abstinence from alcohol abuse, quitting smoking, or starting regular exercise, demonstrated significant association with a lower risk of subsequent SH events, compared to persistence of unhealthy lifestyle behaviors. Moreover, starting unhealthy lifestyle habits was as harmful as maintaining them (Fig. 2). Therefore, intensive individualized education programs need to include this information on lifestyle modification for high-risk patients with SH in T2DM and encourage them to maintain a healthy lifestyle.
CONCLUSIONS
- In summary, SH is a critical issue in T2DM, especially in high-risk populations. Clinicians should ask patients about hypoglycemic events at every visit and pay close attention to this issue. The identification of high-risk patients, intensive individualized education, and frequent monitoring are key factors for preventing SH. In addition to the management of traditional risk factors for SH, adherence to a healthy lifestyle should be emphasized to reduce the development of SH events. Closer adherence to healthy lifestyle factors and changes from unhealthy to healthy lifestyle habits are probably helpful for preventing SH in individuals with T2DM. Therefore, a more patient-centered detailed approach based on clinical evidence needs to be developed for T2DM patients at high risk for SH.
ARTICLE INFORMATION
-
Ethical statements
Not applicable.
-
Conflicts of interest
The author has no conflicts of interest to declare.
-
Funding
None.
Fig. 1.Trends in the prevalence of severe hypoglycemia in patients with type 2 diabetes mellitus in Korea between 2002 and 2019 using the Korean National Health Insurance Service database (shown as gray bars). Severe hypoglycemia was more prevalent in female patients (red dotted line), and dramatically increased with age.
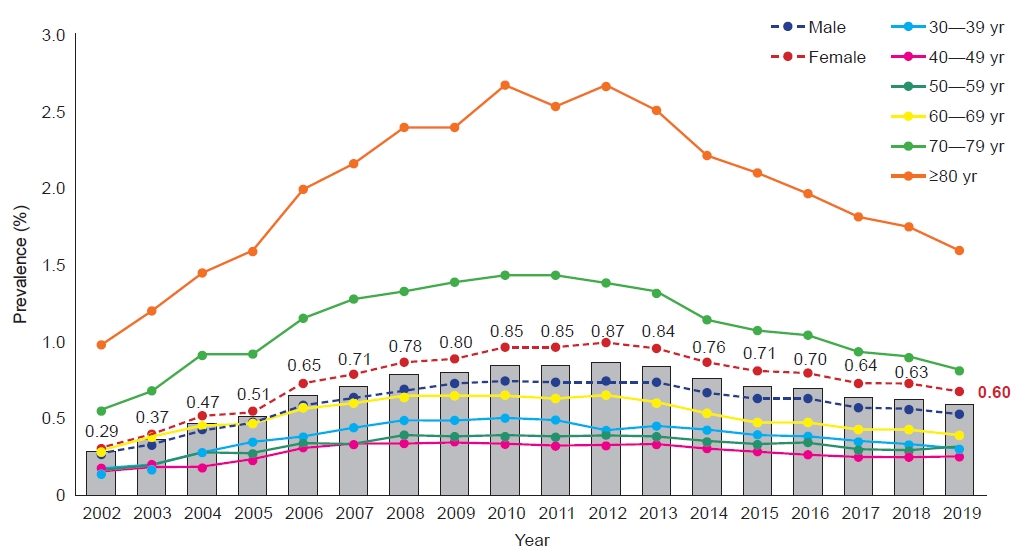
Fig. 2.Severe hypoglycemia (SH) incidence according to the change in each lifestyle behavior in patients with type 2 diabetes mellitus in Korea. In addition to adherence to a healthy lifestyle, any improvement in unhealthy lifestyle factors between the two consecutive health examinations was significantly associated with a lower risk of a subsequent SH event. For example, in case of smoking, compared to nonsmokers for the study period, the hazard ratios for SH in patients with type 2 diabetes mellitus who started smoking, stopped smoking, and maintained smoking were 1.32, 1.17, and 1.30, respectively. Unhealthy lifestyle factors are current smoking, heavy alcohol consumption (≥30 g/day), or lack of regular exercise (moderate-intensity physical activity for <30 min/day, <5 times/wk or strenuous-intensity physical activity for <20 min/day, <3 times/wk). The values are presented as hazard ratio (95% confidence interval).
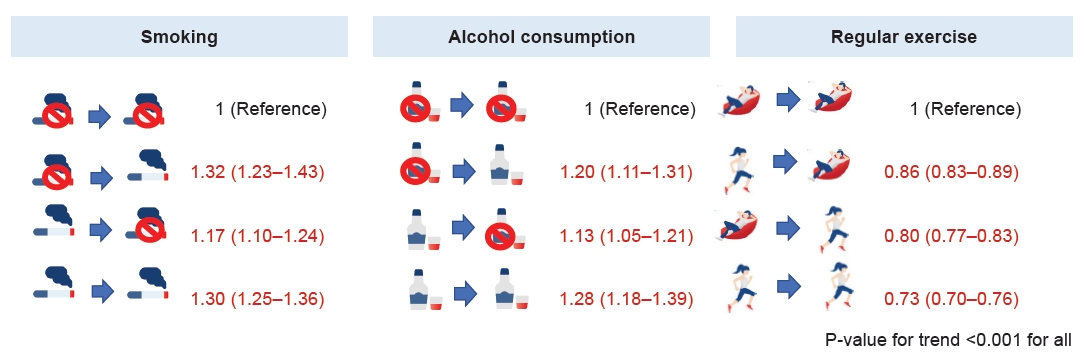
Table 1.Recommended classification of hypoglycemia in diabetes
|
Level |
Glycemic criteria |
Clinical description |
|
1 |
54 to <70 mg/dL |
Clinically important hypoglycemia independent of the severity of hypoglycemic symptoms; should be treated with glucose |
|
2 |
<54 mg/dL |
Sufficiently low to indicate serious, clinically important hypoglycemia |
|
3 |
No specific glucose level |
A severe event characterized by altered mental and/or physical functioning that requires assistance from another person for recovery |
REFERENCES
- 1. American Diabetes Association Professional Practice Committee, Draznin B, Aroda VR, Bakris G, Benson G, Brown FM, et al. 6. Glycemic targets: standards of medical care in diabetes: 2022. Diabetes Care 2022;45(Suppl 1):S83–96.Article
- 2. Frier BM. Hypoglycaemia in diabetes mellitus: epidemiology and clinical implications. Nat Rev Endocrinol 2014;10:711–22.ArticlePubMedPDF
- 3. Hemmingsen B, Lund SS, Gluud C, Vaag A, Almdal T, Hemmingsen C, et al. Intensive glycaemic control for patients with type 2 diabetes: systematic review with meta-analysis and trial sequential analysis of randomised clinical trials. BMJ 2011;343:d6898. ArticlePubMedPMC
- 4. Pawaskar M, Witt EA, Engel SS, Rajpathak SN, Iglay K. Severity of hypoglycaemia and health-related quality of life, work productivity and healthcare costs in patients with type 2 diabetes in Europe. Endocrinol Diabetes Metab 2018;1:e00011.ArticlePubMedPMCPDF
- 5. International Hypoglycaemia Study Group. Glucose concentrations of less than 3.0 mmol/L (54 mg/dL) should be reported in clinical trials: a joint position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2017;40:155–7.ArticlePubMedPDF
- 6. Choi SY, Ko SH. Severe hypoglycemia as a preventable risk factor for cardiovascular disease in patients with type 2 diabetes mellitus. Korean J Intern Med 2021;36:263–70.ArticlePubMedPMCPDF
- 7. Lacy ME, Gilsanz P, Eng C, Beeri MS, Karter AJ, Whitmer RA. Severe hypoglycemia and cognitive function in older adults with type 1 diabetes: the Study of Longevity in Diabetes (SOLID). Diabetes Care 2020;43:541–8.ArticlePubMedPMCPDF
- 8. Cryer PE. Individualized glycemic goals and an expanded classification of severe hypoglycemia in diabetes. Diabetes Care 2017;40:1641–3.ArticlePubMedPDF
- 9. Seaquist ER, Anderson J, Childs B, Cryer P, Dagogo-Jack S, Fish L, et al. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society. Diabetes Care 2013;36:1384–95.ArticlePubMedPMCPDF
- 10. Yun JS, Han K, Ko SH. Trends of severe hypoglycemia in patients with type 2 diabetes in Korea: a longitudinal nationwide cohort study. J Diabetes Investig 2022;Mar 9 [Epub]. https://doi.org/10.1111/jdi.13786.Article
- 11. Bae JH, Han KD, Ko SH, Yang YS, Choi JH, Choi KM, et al. Diabetes fact sheet in Korea 2021. Diabetes Metab J 2022;46:417–26.ArticlePubMedPMCPDF
- 12. Jensen MH, Kjolby M, Hejlesen O, Jakobsen PE, Vestergaard P. Risk of major adverse cardiovascular events, severe hypoglycemia, and all-cause mortality for widely used antihyperglycemic dual and triple therapies for type 2 diabetes management: a cohort study of all Danish users. Diabetes Care 2020;43:1209–18.ArticlePubMedPDF
- 13. Baek JH, Yang YS, Ko SH, Han KD, Kim JH, Moon MK, et al. Real-world prescription patterns and barriers related to the use of sodium-glucose cotransporter 2 inhibitors among Korean patients with type 2 diabetes mellitus and cardiovascular disease. Diabetes Metab J 2022;Jun 3 [Epub]. https://doi.org/10.4093/dmj.2022.0002.Article
- 14. Hur KY, Moon MK, Park JS, Kim SK, Lee SH, Yun JS, et al. 2021 Clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J 2021;45:461–81.ArticlePubMedPMCPDF
- 15. Yun JS, Ko SH. Current trends in epidemiology of cardiovascular disease and cardiovascular risk management in type 2 diabetes. Metabolism 2021;123:154838. ArticlePubMed
- 16. Pieber TR, Marso SP, McGuire DK, Zinman B, Poulter NR, Emerson SS, et al. DEVOTE 3: temporal relationships between severe hypoglycaemia, cardiovascular outcomes and mortality. Diabetologia 2018;61:58–65.ArticlePubMedPMCPDF
- 17. Standl E, Stevens SR, Lokhnygina Y, Bethel MA, Buse JB, Gustavson SM, et al. Confirming the bidirectional nature of the association between severe hypoglycemic and cardiovascular events in type 2 diabetes: insights from EXSCEL. Diabetes Care 2020;43:643–52.ArticlePubMedPDF
- 18. Cha SA, Yun JS, Lim TS, Hwang S, Yim EJ, Song KH, et al. Severe hypoglycemia and cardiovascular or all-cause mortality in patients with type 2 diabetes. Diabetes Metab J 2016;40:202–10.ArticlePubMedPMCPDF
- 19. Zaccardi F, Ling S, Lawson C, Davies MJ, Khunti K. Severe hypoglycaemia and absolute risk of cause-specific mortality in individuals with type 2 diabetes: a UK primary care observational study. Diabetologia 2020;63:2129–39.ArticlePubMedPMCPDF
- 20. Rana JS, Moffet HH, Liu JY, Karter AJ. Severe hypoglycemia and risk of atherosclerotic cardiovascular disease in patients with diabetes. Diabetes Care 2021;44:e40–1.ArticlePubMedPMCPDF
- 21. Lee AK, Warren B, Lee CJ, McEvoy JW, Matsushita K, Huang ES, et al. The association of severe hypoglycemia with incident cardiovascular events and mortality in adults with type 2 diabetes. Diabetes Care 2018;41:104–11.ArticlePubMedPMCPDF
- 22. Malik AH, Yandrapalli S, Aronow WS, Jain D, Frishman WH, Panza JA, et al. Severe hypoglycemia and risk of subsequent cardiovascular events: systematic review and meta-analysis of randomized controlled trials. Cardiol Rev 2020;28:244–9.ArticlePubMed
- 23. Yun JS, Park YM, Han K, Cha SA, Ahn YB, Ko SH. Severe hypoglycemia and the risk of cardiovascular disease and mortality in type 2 diabetes: a nationwide population-based cohort study. Cardiovasc Diabetol 2019;18:103. ArticlePubMedPMCPDF
- 24. Nishioka Y, Okada S, Noda T, Myojin T, Kubo S, Ohtera S, et al. Absolute risk of acute coronary syndrome after severe hypoglycemia: a population-based 2-year cohort study using the National Database in Japan. J Diabetes Investig 2020;11:426–34.ArticlePubMedPMCPDF
- 25. Nuzzo A, Brignoli A, Ponziani MC, Zavattaro M, Prodam F, Castello LM, et al. Aging and comorbidities influence the risk of hospitalization and mortality in diabetic patients experiencing severe hypoglycemia. Nutr Metab Cardiovasc Dis 2022;32:160–6.ArticlePubMed
- 26. Ko SH, Park YM, Yun JS, Cha SA, Choi EK, Han K, et al. Severe hypoglycemia is a risk factor for atrial fibrillation in type 2 diabetes mellitus: nationwide population-based cohort study. J Diabetes Complications 2018;32:157–63.ArticlePubMedPMC
- 27. Mylona M, Liatis S, Anastasiadis G, Kapelios C, Kokkinos A. Severe iatrogenic hypoglycaemia requiring medical assistance is associated with concurrent prolongation of the QTc interval. Diabetes Res Clin Pract 2020;161:108038. ArticlePubMed
- 28. Cha SA, Yun JS, Lim TS, Kang YG, Lee KM, Song KH, et al. Baseline-corrected QT (QTc) interval is associated with prolongation of QTc during severe hypoglycemia in patients with type 2 diabetes mellitus. Diabetes Metab J 2016;40:463–72.ArticlePubMedPMCPDF
- 29. Kaze AD, Yuyun MF, Erqou S, Fonarow GC, Echouffo-Tcheugui JB. Severe hypoglycemia and incidence of QT interval prolongation among adults with type 2 diabetes. J Clin Endocrinol Metab 2022;107:e2743–50.ArticlePubMedPMCPDF
- 30. Echouffo-Tcheugui JB, Kaze AD, Fonarow GC, Dagogo-Jack S. Severe hypoglycemia and incident heart failure among adults with type 2 diabetes. J Clin Endocrinol Metab 2022;107:e955–62.ArticlePubMedPDF
- 31. Christensen TF, Tarnow L, Randlov J, Kristensen LE, Struijk JJ, Eldrup E, et al. QT interval prolongation during spontaneous episodes of hypoglycaemia in type 1 diabetes: the impact of heart rate correction. Diabetologia 2010;53:2036–41.ArticlePubMedPDF
- 32. Chow E, Bernjak A, Williams S, Fawdry RA, Hibbert S, Freeman J, et al. Risk of cardiac arrhythmias during hypoglycemia in patients with type 2 diabetes and cardiovascular risk. Diabetes 2014;63:1738–47.ArticlePubMedPDF
- 33. Reno CM, Daphna-Iken D, Chen YS, VanderWeele J, Jethi K, Fisher SJ. Severe hypoglycemia-induced lethal cardiac arrhythmias are mediated by sympathoadrenal activation. Diabetes 2013;62:3570–81.ArticlePubMedPMCPDF
- 34. Reno CM, Bayles J, Huang Y, Oxspring M, Hirahara AM, Dosdall DJ, et al. Severe hypoglycemia-induced fatal cardiac arrhythmias are mediated by the parasympathetic nervous system in rats. Diabetes 2019;68:2107–19.ArticlePubMedPMCPDF
- 35. Joy NG, Tate DB, Younk LM, Davis SN. Effects of acute and antecedent hypoglycemia on endothelial function and markers of atherothrombotic balance in healthy humans. Diabetes 2015;64:2571–80.ArticlePubMedPMCPDF
- 36. Dandona P, Chaudhuri A, Dhindsa S. Proinflammatory and prothrombotic effects of hypoglycemia. Diabetes Care 2010;33:1686–7.ArticlePubMedPMCPDF
- 37. Wright RJ, Newby DE, Stirling D, Ludlam CA, Macdonald IA, Frier BM. Effects of acute insulin-induced hypoglycemia on indices of inflammation: putative mechanism for aggravating vascular disease in diabetes. Diabetes Care 2010;33:1591–7.ArticlePubMedPMC
- 38. Echouffo-Tcheugui JB, Daya N, Lee AK, Tang O, Ndumele CE, Windham BG, et al. Severe hypoglycemia, cardiac structure and function, and risk of cardiovascular events among older adults with diabetes. Diabetes Care 2021;44:248–54.ArticlePubMedPMCPDF
- 39. Huang L, Zhou Y, Chen Z, Zhang M, Zhan Z, Wang L, et al. Severe hypoglycemia exacerbates myocardial dysfunction and metabolic remodeling in diabetic mice. Mol Cell Endocrinol 2020;503:110692. ArticlePubMed
- 40. Yun JS, Kim JH, Song KH, Ahn YB, Yoon KH, Yoo KD, et al. Cardiovascular autonomic dysfunction predicts severe hypoglycemia in patients with type 2 diabetes: a 10-year follow-up study. Diabetes Care 2014;37:235–41.ArticlePubMedPDF
- 41. Han K, Yun JS, Park YM, Ahn YB, Cho JH, Cha SA, et al. Development and validation of a risk prediction model for severe hypoglycemia in adult patients with type 2 diabetes: a nationwide population-based cohort study. Clin Epidemiol 2018;10:1545–59.ArticlePubMedPMCPDF
- 42. Davis SN, Duckworth W, Emanuele N, Hayward RA, Wiitala WL, Thottapurathu L, et al. Effects of severe hypoglycemia on cardiovascular outcomes and death in the Veterans Affairs Diabetes Trial. Diabetes Care 2019;42:157–63.ArticlePubMedPMCPDF
- 43. Misra-Hebert AD, Pantalone KM, Ji X, Milinovich A, Dey T, Chagin KM, et al. Patient characteristics associated with severe hypoglycemia in a type 2 diabetes cohort in a large, integrated health care system from 2006 to 2015. Diabetes Care 2018;41:1164–71.ArticlePubMedPDF
- 44. Matsuhisa M, Kuroda A. New risk factors of severe hypoglycemia. J Diabetes Investig 2019;10:219–20.ArticlePubMedPMCPDF
- 45. Namba M, Iwakura T, Nishimura R, Akazawa K, Matsuhisa M, Atsumi Y, et al. The current status of treatment-related severe hypoglycemia in Japanese patients with diabetes mellitus: a report from the committee on a survey of severe hypoglycemia in the Japan Diabetes Society. J Diabetes Investig 2018;9:642–56.ArticlePubMedPMCPDF
- 46. Settles J, Kan H, Child CJ, Gorritz M, Multani JK, McGuiness CB, et al. Previously unrecognized risk factors for severe hypoglycaemia requiring emergency medical care in insulin-treated type 2 diabetes: results from a real-world nested case-control study. Diabetes Obes Metab 2022;24:1235–44.ArticlePubMedPMCPDF
- 47. Yun JS, Han K, Park YM, Han E, Lee YH, Ko SH, et al. Adherence to healthy lifestyle behaviors as a preventable risk factor for severe hypoglycemia in people with type2 diabetes: a longitudinal nationwide cohort study. J Diabetes Investig 2022;Apr 27 [Epub]. https://doi.org/10.1111/jdi.13818.Article
- 48. Avogaro A, Beltramello P, Gnudi L, Maran A, Valerio A, Miola M, et al. Alcohol intake impairs glucose counterregulation during acute insulin-induced hypoglycemia in IDDM patients: evidence for a critical role of free fatty acids. Diabetes 1993;42:1626–34.ArticlePubMed
- 49. Kerr D, Cheyne E, Thomas P, Sherwin R. Influence of acute alcohol ingestion on the hormonal responses to modest hypoglycaemia in patients with type 1 diabetes. Diabet Med 2007;24:312–6.ArticlePubMed
- 50. Bott S, Shafagoj YA, Sawicki PT, Heise T. Impact of smoking on the metabolic action of subcutaneous regular insulin in type 2 diabetic patients. Horm Metab Res 2005;37:445–9.ArticlePubMed
- 51. Tweed JO, Hsia SH, Lutfy K, Friedman TC. The endocrine effects of nicotine and cigarette smoke. Trends Endocrinol Metab 2012;23:334–42.ArticlePubMedPMC
- 52. Satre DD, Gordon NP, Weisner C. Alcohol consumption, medical conditions, and health behavior in older adults. Am J Health Behav 2007;31:238–48.ArticlePubMedPMC
- 53. Arnott C, Li Q, Kang A, Neuen BL, Bompoint S, Lam CS, et al. Sodium-glucose cotransporter 2 inhibition for the prevention of cardiovascular events in patients with type 2 diabetes mellitus: a systematic review and meta-analysis. J Am Heart Assoc 2020;9:e014908.ArticlePubMedPMC
- 54. Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016;375:311–22.ArticlePubMedPMC
- 55. Tsapas A, Avgerinos I, Karagiannis T, Malandris K, Manolopoulos A, Andreadis P, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes: a systematic review and network meta-analysis. Ann Intern Med 2020;173:278–86.ArticlePubMed
- 56. International Hypoglycaemia Study Group. Minimizing hypoglycemia in diabetes. Diabetes Care 2015;38:1583–91.ArticlePubMedPDF
Citations
Citations to this article as recorded by




 PubReader
PubReader ePub Link
ePub Link Cite
Cite