Dose Selection of Non-Vitamin K Antagonist Oral Anticoagulants in Korean Patients with Non-Valvular Atrial Fibrillation
Article information

Abstract
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia. In the Asian population, patients with AF have been shown to have increased risks of ischemic stroke and all-cause death compared to patients without AF by 3.34- and 2.61-fold, respectively. AF guidelines recommend oral anticoagulation (OAC) therapy in AF patients with a CHA2DS2-VASc score of ≥1 for men and ≥2 for women with non-valvular AF. After the introduction of non-vitamin K antagonist oral anticoagulants (NOACs) as a treatment for AF, their use has become widespread. Compared to warfarin, NOACs showed comparable efficacy for the prevention of thromboembolic events and superior safety in terms of bleeding complications, especially intracranial hemorrhage. Physicians should keep in mind considerations for optimal OAC therapy to achieve the best outcome. Furthermore, appropriate dose selection in order to achieve the best clinical outcome is an important issue in clinical practice. All NOACs do not have the same rules for dose reduction, and dose reduction of NOACs is primarily recommended according to the dose reduction criteria investigated in pivotal randomized control trials. In this review, we focus on the optimal dose of NOAC and summarize current guidelines and evidence for appropriate dosing of NOACs.
INTRODUCTION
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia. The global prevalence of AF is increasing, and with this occurs a significant increase in the burden of AF-related healthcare.1-3) According to a recent study in the Asian population, patients with AF had increased risks of ischemic stroke and all-cause death compared to patients without AF by 3.34- and 2.61-fold, respectively.4) To prevent these adverse events and to improve clinical outcomes of patients with AF, guidelines recommend oral anticoagulation (OAC) therapy in patients with a CHA2DS2-VASc score of ≥1 for men and ≥2 for women with nonvalvular AF.5-8) For decades, vitamin K antagonists (i.e., warfarin) were the only available anticoagulant; however, non-vitamin K antagonist oral anticoagulants (NOACs) have recently been introduced into clinical practice. Compared to warfarin, NOACs showed comparable efficacy for the prevention of thromboembolic events and superior safety in terms of bleeding complications, especially intracranial hemorrhage (ICH).9) After the introduction of NOACs as a treatment for AF, the use of NOACs is now widespread.10-12) Although the use of NOACs has generally been shown to improve clinical outcomes in patients with non-valvular AF,13) physicians should keep in mind considerations for optimal OAC therapy to achieve the best outcome as follows: 1) identification of truly low-risk patients who do not need OAC therapy; 2) OAC therapy if patients are not “truly low-risk patients”; 3) NOACs are recommended in preference to warfarin except special contraindications such as moderate to severe mitral stenosis or prosthetic valve implantation; 4) better NOAC according to patient profiles; 5) right dose of NOAC; and 6) good drug adherence.14) In this review, we focus on obtaining the “right dose of NOAC” summarize current guidelines and evidence for appropriate dosing, identify gaps between knowledge and real-world practice in NOAC dosing, and introduce future studies for the evaluation of appropriate dose of NOACs in Asian patients with AF.
DOSE TESTED IN THE PIVOTAL RANDOMIZED CLINICAL TRIALS OF NOACS AND PRESPECIFIED DOSE REDUCTION CRITERIA OF NOACS IN CLINICAL TRIALS
Currently, 4 NOACs are available: dabigatran, rivaroxaban, apixaban, and edoxaban. In the pivotal randomized clinical trial (RCT) of each NOAC versus warfarin, standard and reduced doses were tested. In the RE-LY trial,15) patients were randomized into 3 groups as follows: dabigatran 150 mg twice daily (n=6,075), 110 mg twice daily (n=6,015), and warfarin (n=6,022); there was no prespecified dose reduction criteria for dabigatran. In the Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKETAF) trial,16) rivaroxaban given at 20 mg once daily was the standard dose; patients with a creatinine clearance (CrCl) <50 mL/min received a reduced dose of rivaroxaban (15 mg once daily). Among the total study population who received rivaroxaban (n=7,131), 21% of patients received rivaroxaban 15 mg once daily. In the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial,17) the standard dose of apixaban was 5 mg twice daily and 2.5 mg apixaban twice daily was prescribed in a subset of patients with 2 or more of the following criteria: age ≥80 years, body weight ≤60 kg, or serum creatinine levels ≥1.5 mg/dL. Of the 9,120 patients receiving apixaban, only 4.7% were prescribed 2.5 mg of apixaban. In the Effective Anticoagulation With Factor Xa Next Generation in Atrial Fibrillation–Thrombolysis in Myocardial Infarction 48 (ENGAGE AF-TIMI 48) trial,18) patients were assigned to either a high dose edoxaban regimen (60/30 mg once daily, n=7,035), low dose edoxaban regimen (30/15 mg once daily, n=7,034), and warfarin (n=7,036) at a 1:1:1 ratio. Following the findings of this study, the high-dose edoxaban regimen (60/30 mg once daily) was finally approved for stroke prevention in patients with AF. In the high dose edoxaban regimen group, edoxaban given at 60 mg once daily was the standard does. The dose was halved (30 mg once daily) if any of the following characteristics were present: estimated CrCl ≤50 mL/min, body weight ≤60 kg, or the concomitant use of verapamil or quinidine (potent P-glycoprotein inhibitors). Of the 7,035 patients in the high dose edoxaban regimen group, 25.4% of patients received the reduced dose. Table 1 summarizes the dose reduction criteria of the 4 NOACs in pivotal RCTs. Korean labels adopted the dose reduction criteria of the pivotal RCTs with the exception of dabigatran. For dabigatran, in line with the 2016 European Society of Cardiology (ESC) AF management guidelines, a reduced dose (110 mg twice daily) may be considered in patients >75 years old (Table 1).5)19)
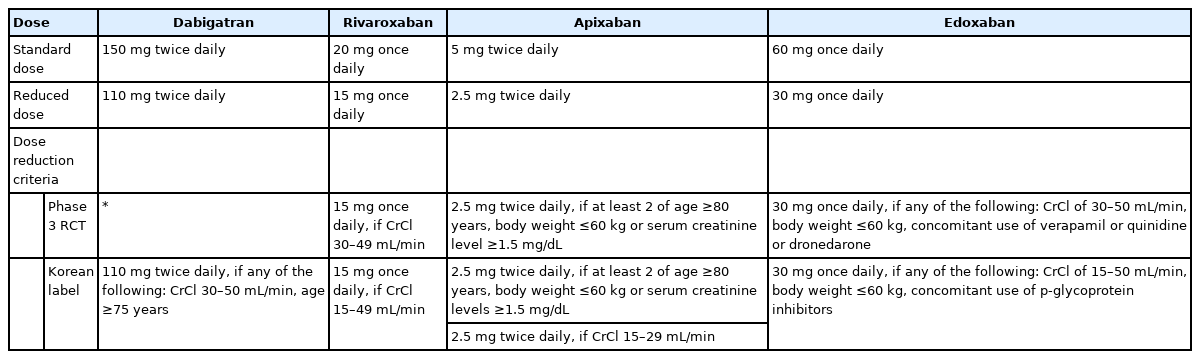
Dose reduction criteria of 4 NOACs from pivotal RCTs
GUIDELINE RECOMMENDATION FOR APPROPRIATE DOSING OF NOACS
In the 2016 ESC guidelines, the dose reduction criteria of each NOAC from the pivotal RCT were introduced.5) For dabigatran, 110 mg twice daily was recommended for patients older than 75 years or patients at high-risk of gastrointestinal bleeding.5) In the 2019 American Heart Association (AHA)/American College of Cardiology (ACC)/Heart Rhythm Society (HRS) guidelines, dose adjustments of NOACs were advised to be made according to Food and Drug Administration (FDA) dosing guidelines.6) When considering double therapy (P2Y12 inhibitors and NOAC), a reduced dose of rivaroxaban (15 mg once daily) is recommended.6) In the 2018 American College of Chest Physicians (ACCP) guidelines, label-adjusted NOAC dosing is generally recommended in correlation with dose reduction criteria from the pivotal RCTs.7) The 2018 European Heart Rhythm Association (EHRA) practical guide on the use of NOACs also follows this consensus.14) A dose reduction of NOACs is primarily recommended according to the dose reduction criteria investigated in the pivotal RCTs.
In the 2018 Korean guidelines, based on the dose reduction criteria outlined in the pivotal RCTs, a few additional conditions for dose reduction are suggested.8) For dabigatran, patients with CrCl of 30 to 50 mL/min, concomitant medications (p-glycoprotein inhibitors, antiplatelets, and non-steroidal anti-inflammatory drugs), increased bleeding risk (coagulopathy, thrombocytopenia, platelet dysfunction, recent major trauma or biopsy, and infective endocarditis), or age ≥75 years the recommendation is a reduced dose of dabigatran (110 mg twice daily). For rivaroxaban, for a CrCl <50 ml/min and patients aged ≥80 years the recommendation is a reduced dose of rivaroxaban (15 mg once daily). These age cut-offs for dose reduction have limited evidence. Further investigation is required to develop comprehensive evidence for these recommendations.
REAL-WORLD PRACTICE IN ASIAN POPULATION
As previously discussed, the same dose reduction rules do not apply to all NOACs (Table 1), thus, choosing the correct dose is challenging in daily clinical practice. A certain proportion of patients receiving NOACs do not receive on-label dosing.20)21) In the U.S. the prospective registry for AF patients receiving NOACs (n=5,738) states that 87% of patients were prescribed on-label dosed NOACs, whilst 9.4% were underdosed, and 3.4% were overdosed.20)
In the Asian population, reduced doses of NOACs were mainly prescribed to patients with AF, and the use of such doses was considerably more common in the Asian population than in the non-Asian population (Table 2).22-38) There are several potential reasons for the more frequent use of reduced dose NOACs in Asian patients with AF. First, Asians generally have a lower body weight and smaller body size than non-Asians, who were represented to a greater degree in the pivotal RCTs.28) Second, Asians were shown to have a higher risk of ICH than non-Asians in the warfarin era.39) Physicians may tend to be more conservative than aggressive in an attempt to avoid adverse bleeding events when they prescribe OAC therapy for patients with AF. Third, in Japan, based on pharmacokinetic data of the Japanese elderly, a standard dose of rivaroxaban is 15 mg once daily and rivaroxaban 10 mg once daily is prescribed for patients with renal impairment as a reduced dose.40) The J-ROCKET trial had some limitations in its attempt to determine which is the optimal standard dose of rivaroxaban for Asian patients with AF (rivaroxaban 20 mg vs. 15 mg). A small number of patients were enrolled, and the common comparator for evaluating efficacy and safety was warfarin. To select an optimal standard dose of rivaroxaban, a direct comparison between rivaroxaban given at 20 mg and at 15 mg in patients with a CrCl ≥50 mL/min. Although further evidence is needed in order for 15 mg of rivaroxaban as a standard dose for Asians to be accepted, the results of the J-ROCKET trial might influence the real-world clinical practice in other Asian countries.22)30)41)
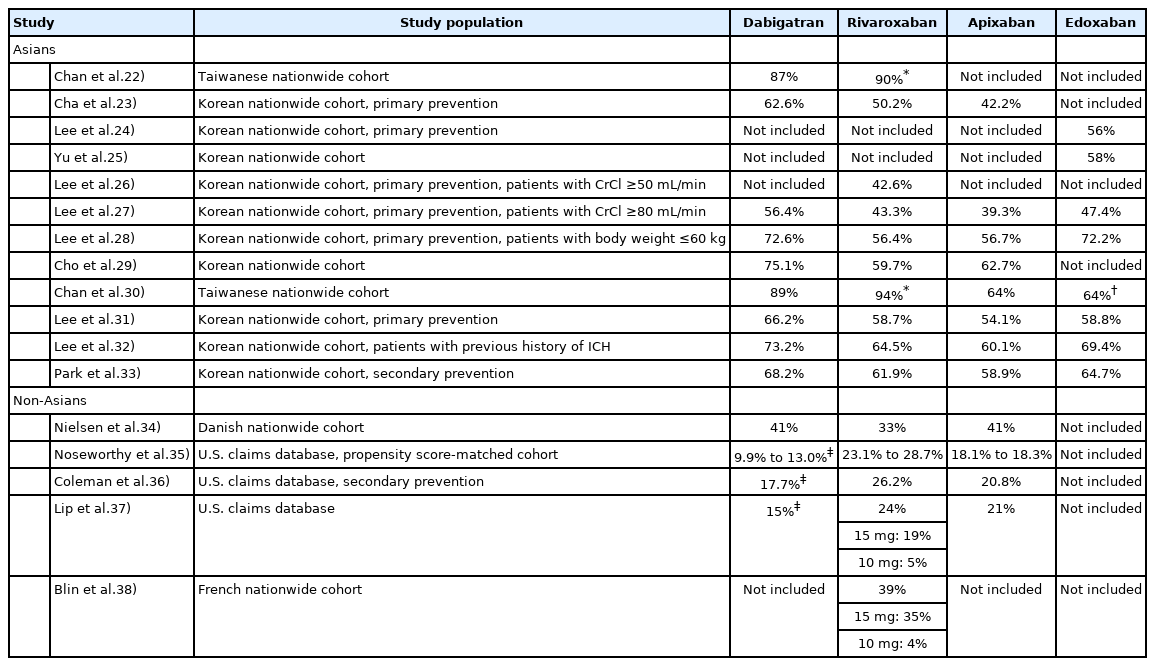
The proportion of use of reduced dose of NOACs in real-world observational studies
There might be a discrepancy between patients receiving reduced doses of NOACs and patients receiving an off-label underdose of NOACs. To identify not merely a reduced dose but an off-label underdose of NOACs, information including body weight, renal function, age, and concomitant drugs need to be available. In nationwide observational registries, this information is partly available. Therefore, data regarding off-label dosing of NOAC in Asian patients with AF is still limited. From a large-scale prospective registry of Korean patients with AF, the COmparison study of Drugs for symptom control and complication prEvention of AF (CODE-AF) registry, we found that a substantial proportion of Korean patients with AF received an off-label underdose of NOACs as follows: 36.4% of total NOAC users, 1.8% of dabigatran users, 53.9% of rivaroxaban users, 55% of apixaban users, and 23.5% of edoxaban users.42) According to this study, only a small proportion of patients (1.6% of total NOAC users) received an off-label overdose of NOACs. Of the 4 NOACs, apixaban and rivaroxaban were most likely to be prescribed as an off-label underdose; 83% of patients treated with apixaban 2.5 mg twice daily and 78% of patients treated with rivaroxaban 15 mg once daily were identified as users of NOAC that had the dose inappropriately reduced (off-label underdose). The risk factors for receiving an off-label underdose of NOACs were old age (≥75 years), female sex, low body weight (≤60 kg), renal impairment (CrCl ≤50 mL/min), hypertension, previous bleeding history, and concomitant medication such as antiplatelet agents or dronedarone.42)
CLINICAL IMPACT OF OFF-LABEL DOSING OF NOACS
As described above, the use of reduced-dose NOACs is widespread in clinical practice in the Asian population. Regardless of label adherence to NOAC dosing, Asian observational retrospective data showed a consistent benefit of NOAC compared to warfarin.22-33)41) However, this should not be interpreted as considering the unconditional use of reduced doses of NOACs in Asians to be allowed. The common comparator of these real-world studies was warfarin. The treatment quality of the warfarin group was not collected and or well-controlled for in real-world practice. Even in the pivotal RCTs, the treatment quality of the warfarin group in Asian countries was relatively low.43)
In a recent meta-analysis, patients who received a reduced dose of NOAC in the pivotal RCTs showed comparable efficacy and superior safety compared with warfarin, and these results were consistent with the relative benefit observed in the comparison between full dose NOAC and warfarin.44) Namely, although patients eligible for a reduced dose of NOACs generally had an elevated risk of thromboembolic and hemorrhagic complications, appropriately dose-adjusted NOACs showed a consistent benefit-harm profile compared with warfarin.
In real-world practice, off-label dosing of NOACs, both under and overdosing, was associated with an increased risk for adverse events.20) In each NOAC, the hazards of off-label underdosed rivaroxaban and dabigatran were not significant; however, the use of off-label underdosed apixaban was associated with a nearly 5-fold higher risk of stroke.45) Furthermore, the use of off-label underdosed apixaban showed a similar risk of major bleeding compared with standard-dose apixaban. These previous studies mainly included the non-Asian population. Recently, several studies about label-adherence of NOAC dosing have been reported in the Korean population. The use of reduced dose apixaban in non-eligible patients (those aged under 75 years and without chronic kidney disease) attenuated the benefit observed in the comparison between a standard dose apixaban and warfarin.29) In patients with AF and those who were underweight (≤60 kg), on-label dosing of NOACs showed the best net clinical benefit.26) In patients who were eligible (CrCl ≥50 mL/min), both on-label rivaroxaban 20 mg once daily and off-label underdosed rivaroxaban 15 mg once daily, showed better effectiveness and safety than warfarin.26) On-label rivaroxaban given at 20 mg had a better net clinical benefit compared to off-label underdosed rivaroxaban given at 15 mg use in patients with CrCl ≥50 mL/min. Furthermore, along with the risk of adverse events, off-label underdosed NOAC was also associated with increased stroke severity than that of on-label standard doses or warfarin given at a therapeutic intensity.46) Overall, previous studies consistently showed that the use of off-label underdosed NOACs attenuated the benefit of NOACs over warfarin.
KNOWLEDGE GAPS AND UNMET NEEDS FOR CHOOSING AN APPROPRIATE DOSE OF NOACS IN ASIAN PATIENTS WITH AF AND FUTURE STUDIES
Despite published literation, knowledge gaps and unmet needs remain with regards to appropriate doses for NOACs in Asian patients with AF. Although Yao et al.45) reported off-label underdosed apixaban increased the risk of ischemic stroke, these findings were not reproducible or consistently reported, especially in the Asian population. Furthermore, one of the difficulties in evaluating the risk of off-label underdose NOAC use is the clinical characteristics of patients treated with off-label underdose NOACs are similar to patients who are eligible for on-label reduced dose NOACs.20)42)45) In observational studies, we could not fully adjust residual or unrecognized confounding factors between patients treated with on-label standard doses and patients who should have received on-label standard doses but received off-label underdoses, because many factors such as previous minor or major bleeding history or fluctuation in renal function or body weight could affect physicians choices in real-world clinical settings. Ideally, large-scale prospective RCTs should be implanted to answer these questions, however, the stark reality is that there are insufficient resources to conduct RCTs for every important clinical issue.
Although observational studies have several limitations, however, they can play a critical role in “hypothesis-generating.” For example, in previous studies, on-label rivaroxaban given at 20 mg once daily had shown a statistically significant, however modest, benefit compared with off-label rivaroxaban given at 15 mg once daily in patients with CrCl ≥50 mL/min.26) However, in subgroup analyses for patients with marginal CrCl (50 to <60 mL/min), onlabel rivaroxaban given at 20 mg once daily was associated with an increased risk of major bleeding compared to off-label rivaroxaban given at 15 mg once daily. These findings could suggest that “the Asian population requires a more conservative (higher) CrCl cut-off for dose reduction of rivaroxaban” or “physicians need more meticulous monitoring and to enforce more individualized dose reduction in patients at the margin of dose reduction criteria who have the possibility of on-going declining or fluctuating renal function.”
In Korea, ongoing prospective non-interventional registries are pending including the LEDIOS (NCT03554837) and XAIENT (NCT04096547).47)48) Briefly, the LEDIOS registry evaluated the safety and effectiveness of low dose edoxaban in patients with non-valvular AF. The original protocol planned to include patients who received an on-label low dose of edoxaban determined by the patients’ body weight (≤60 kg), creatinine clearance (≤50 mL/min), and concomitant medication. Patients with marginal or fluctuating body weight or renal function close to the dose reduction cut-off could be analyzed in an exploratory analysis. The XAIENT registry evaluated the optimal dose of rivaroxaban in elderly patients with or without renal impairment. Although doses of rivaroxaban (15 mg vs. 20 mg) were not randomly allocated in this study, the efficacy and safety of 15 mg or 20 mg of rivaroxaban in elderly patients (≥65 years) could be evaluated by on- or off-label use in real-world practice.
CONCLUSIONS
NOAC use is widespread for OAC therapy in patients with non-valvular AF and appropriate dose selection to achieve the best clinical outcome is an important issue in the clinical practice. Although current evidence has shown that on-label dosing resulted in the best clinical outcomes, further studies are needed to find optimal doses of NOACs for Asian patients with AF.
Notes
Conflict of Interest
The authors have no financial conflicts of interest.
Author Contributions
Data curation: Lee SR; Project administration: On YK; Writing - original draft: Lee SR, On YK.