Obesity and heart failure with preserved ejection fraction: pathophysiology and clinical significance
Article information

Abstract
Obesity is a risk factor for heart failure and other types of cardiovascular disease. Of particular note, over 80% of patients with heart failure with a preserved ejection fraction (HFpEF) are overweight or obese. In this study, we aimed to review the association between obesity and HFpEF. Obese patients with HFpEF exhibit a distinct phenotype. In addition to impaired left ventricular (LV) diastolic function and high filling pressures, obese patients with HFpEF possess other factors that cause elevated LV filling pressure, such as a greater dependence on plasma volume expansion, aggravated pericardial restraint, and increased ventricular interaction. Obesity can contribute to HFpEF through hemodynamic, neurohormonal, inflammatory, and mechanical mechanisms. An increased amount of body fat can induce plasma volume expansion, resulting in chamber remodeling, pericardial restraint, and ultimately elevations in LV filling pressure. Obesity can mediate the activation of sympathetic nervous system signaling and the renin-angiotensin-aldosterone system. These unique pathophysiological characteristics of individuals with both obesity and HFpEF suggest that obesity with HFpEF can be considered a specific phenotype. Future research is expected to clarify effective treatment modalities for obesity-related HFpEF.
INTRODUCTION
The increasing prevalence of heart failure (HF) has placed a substantial burden on the public health system [1]. The percentage of people with HF is expected to rise from 2.4% in 2012 to 3.0% in 2030 [2,3]. Therefore, identifying modifiable factors that contribute to HF is essential.
Obesity refers to excess fat distribution in the body and is a risk factor for various cardiovascular diseases [4]. Obesity could also affect the pathophysiology of HF more strongly than that of other subtypes of cardiovascular disease, in which obesity-related cardiovascular risk factors are less strongly implicated [5].
Approximately 50% of HF patients have HF with a preserved ejection fraction (HFpEF), meaning that their left ventricular (LV) diastolic function is not impaired [6]. Since the prevalence of overweight or obesity is over 80% in patients with HFpEF, the contribution of obesity to the pathophysiology of HFpEF has been of interest to many researchers [7]. Therefore, we aimed to review the association between obesity and HFpEF.
THE PHENOTYPE OF OBESITY-RELATED HFpEF
Previous studies have defined a distinct phenotype of obesity-related HFpEF, which is a heterogeneous syndrome [8]. Obokata et al. [8] assessed and compared the clinical characteristics of subjects with obesity-related HFpEF to those of nonobese subjects with HFpEF and control subjects without HF. Obese patients with HFpEF exhibited increased plasma volume expansion, more concentric biventricular remodeling, more profound right ventricular (RV) dysfunction, worse exercise competence, more severe hemodynamic disarrangements upon exercise, and weaker pulmonary vasodilation than nonobese subjects with HFpEF and control subjects without HF [8]. In addition to the common findings of impaired LV diastolic function and high filling pressures in HFpEF regardless of adiposity, obese patients with HFpEF possessed other causes of elevated LV filling pressure, such as a greater dependence on plasma volume expansion, aggravated pericardial restraint, and increased ventricular interaction, which could be synergistically amplified with an increasing RV afterload (Fig. 1) [8].
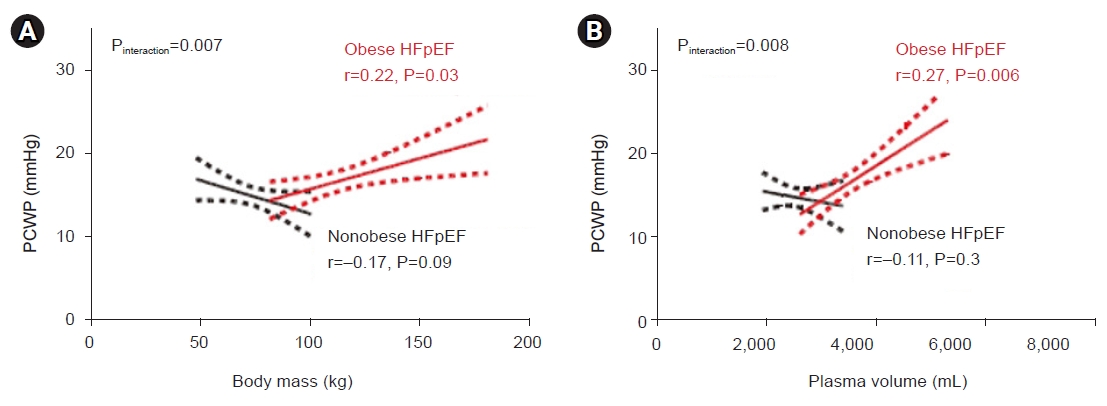
Positive correlations between the left heart filling pressure and (A) body mass and (B) plasma volume in obese heart failure with preserved ejection fraction (HFpEF) but not in nonobese HFpEF. PCWP, pulmonary capillary wedge pressure. Adapted from Obokata et al. [8] with permission from Wolters Kluwer Health Inc.
A secondary analysis of the RELAX (Phosphodiesterase-5 Inhibition to Improve Clinical Status and Exercise Capacity in Heart Failure with Preserved Ejection Fraction) trial, a multicenter randomized clinical trial, displayed that obese HFpEF was related to poor quality of life, severe symptoms of heart failure, enhanced systemic inflammation, impaired exercise capacity, and an elevated metabolic cost of exertion, in comparison with nonobese HFpEF (Fig. 2) [9].
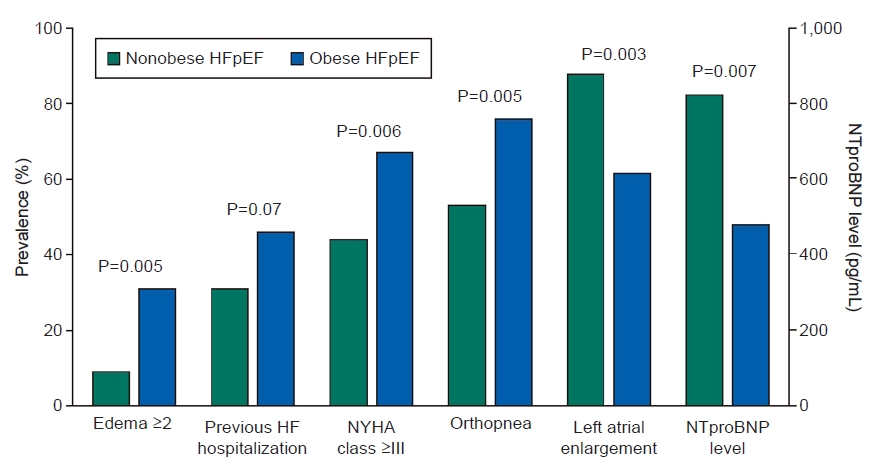
Higher proportion of individuals suffering the symptoms and signs related to heart failure (HF) despite a lower prevalence of left atrial enlargement and lower levels of N-terminal pro B-type natriuretic peptide (NT-proBNP). HFpEF, heart failure with preserved ejection fraction; NYHA, New York Heart Association. Adapted from Reddy et al. [9] with permission from Elsevier.
THE PATHOPHYSIOLOGY OF OBESITY-RELATED CHANGES IN HEART STRUCTURE AND FUNCTION
Obesity can contribute to HFpEF through hemodynamic, neurohormonal, inflammatory, and mechanical mechanisms (Fig. 3) [1]. In obese patients with HFpEF, plasma volume expansion can cause chamber remodeling such as RV dilatation, RV dysfunction, LV hypertrophy, and LV diastolic dysfunction, resulting in pericardial restraint and, finally, elevations in LV filling pressure [8,10–12]. The body fat distribution is more important than the simple quantity of fat mass itself [13]. In particular, obesity-related diastolic dysfunction is more pronounced in individuals with high central or visceral adiposity [14–16]. In addition, excessive systemic vasodilation can occur in response to the increase in plasma volume [8,17–19] and several adipokines released by perivascular adipose tissues [20,21].
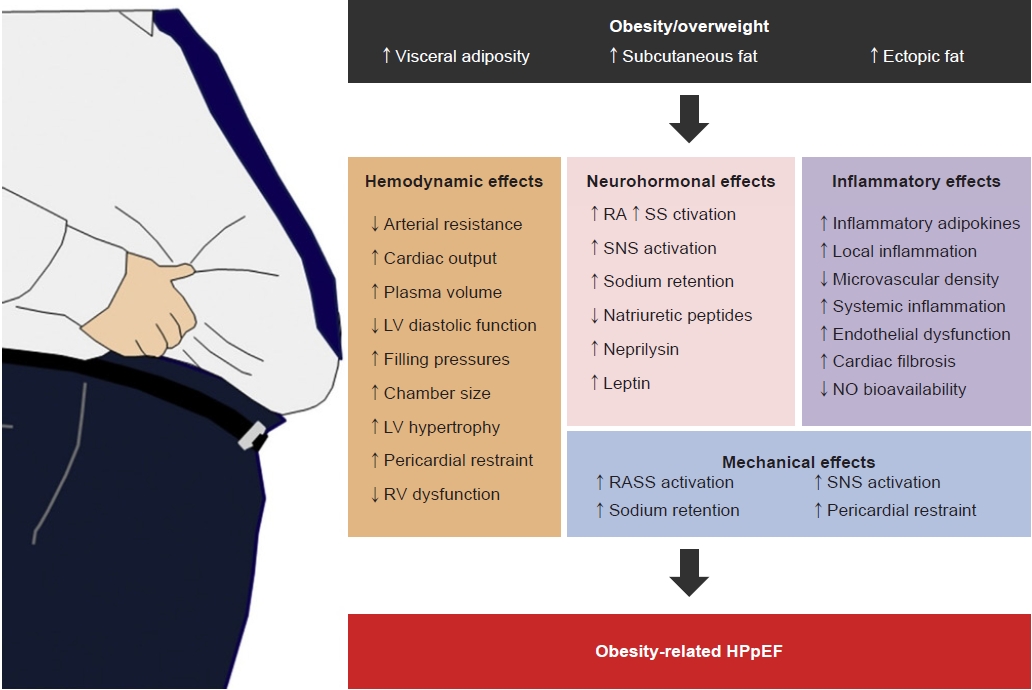
Adverse effects of obesity on the cardiovascular system in heart failure with preserved ejection fraction. LV, left ventricular; RV, right ventricular; RAAS, renin-angiotensin-aldosterone system; SNS, sympathetic nervous system; NO, nitric oxide; HFpEF, heart failure with preserved ejection fraction. Adapted from Harada et al. [1] with permission from Elsevier.
Obesity may mediate neurohormonal activation, such as sympathetic nervous system (SNS) signaling, renin-angiotensin-aldosterone system (RAAS) activation, and an increment of adipokines that can enhance SNS and RAAS activity (e.g., leptin or aldosterone) [19,22]. SNS activation promotes increased sodium reabsorption, leading to blood shift from the splanchnic to the central circulation and exacerbating HF [23].
As a mechanical pathway, the accumulation of visceral, retroperitoneal, and perirenal fat and degradation of natriuretic peptides by adipocytes induce renal sodium reabsorption, resulting in plasma volume expansion [19,24–26].
CONCLUSIONS
Since little effective treatment for HFpEF is available, unlike HF with reduced ejection fraction [27,28], recognizing the significance of obesity in the development of HFpEF may pave the way towards it serving as a key therapeutic target in the future. Individuals with obesity-related HFpEF present unique pathophysiological characteristics, suggesting that obesity with HFpEF can be considered a specific phenotype. Future research is expected to clarify effective treatment modalities for obesity-related HFpEF.
Notes
Ethical statements
Not applicable.
Conflicts of interest
The author has no conflicts of interest to declare.
Funding
None.