Liraglutide, a glucagon-like peptide-1 analog, in individuals with obesity in clinical practice
Article information

Abstract
Obesity is a disease requiring treatment. The prevalence of obesity is steadily increasing both in Korea and worldwide. Individuals with obesity are at elevated risks of diabetes, cerebrovascular disease, and solid cancer; therefore, obesity is now considered to be a disease requiring treatment, rather than merely a cosmetic problem. Nutrition and exercise are the basic forms of obesity management, but it is not easy to lose weight through only one’s own willpower. Accordingly, policies for establishing a cultural environment that encourages desirable behaviors are proposed through multifaceted efforts involving the media and local organizations. However, the pharmacological and surgical treatments selected as medical interventions should be individualized based on an understanding of each individual’s cause of obesity and characteristics. It is important to understand how to enhance and maintain the effectiveness of treatment not only for the prescribing medical staff, but also for the individual with obesity who is being treated.
INTRODUCTION
In general, when we eat, the blood glucose level rises, and the small intestine secretes hormones known as incretins [1]. These hormones work in the liver and pancreas to regulate elevated blood glucose [1]. After the discoveries of the gastrointestinal hormones, secretin in 1902 and gastrin in 1905, there was a time when diabetes was treated by injecting intestinal extract, assuming that gastrointestinal hormones were involved in glycemic control of the pancreas [2]. The results were disappointing at that time, but once it became possible to measure insulin, researchers documented the so-called incretin effect, whereby insulin secretion is increased by oral ingestion of glucose to a greater extent than with intravenous injection. The incretin hormones, glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1 (GLP-1), were discovered after this incretin effect received attention from researchers [2].
In studies related to the incretin effect, when glucose is administered orally or intravenously and the blood glucose level remains the same, the blood insulin concentration increases more from oral administration than from intravenous administration [1]. This demonstrates that hormones secreted from the gastrointestinal tract during oral glucose administration are involved in promoting pancreatic insulin secretion. Specifically, it has been established that 50% to 70% of insulin secretion in response to oral glucose administration is due to the incretin effect [1].
MECHANISM OF THE WEIGHT LOSS EFFECT OF GLP-1 RECEPTOR AGONISTS
The incretin hormones secreted by L cells in the ileum and colon are GLP-1 receptor agonists (RAs) [3]. Fig. 1 shows the effects of GLP-1 RAs on various organs [4].
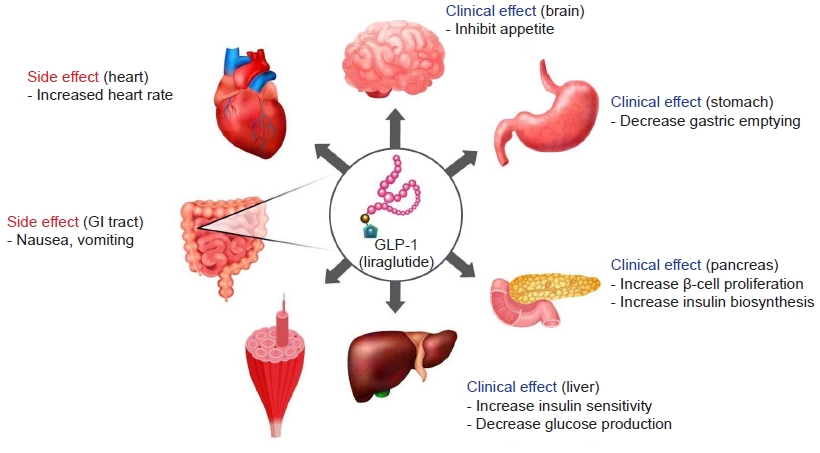
Brain: appetite suppression
In the brain, GLP-1 RAs act on the hypothalamus, which is involved in appetite regulation, to give a feeling of satiety and reduce appetite [5]. A study showed that changes in postprandial GLP-1 RA levels were positively correlated with local cerebral blood flow to the left dorsolateral prefrontal cortex and the hypothalamus, which is known to be associated with satiety and the control of food intake [5]. Another study reported that subjects using liraglutide, a GLP-1 RA, had attenuated responses in the cortex and insular regions of the brain when exposed to images of food in the fasting state compared to the control group [6].
Digestive system: increased satiety
GLP-1 RAs increase satiety by inhibiting gastrointestinal motility [7]. In a study examining gastric emptying after liraglutide administration, when 3.0 mg of liraglutide was used, less gastric emptying occurred during 1 hour than when 1.8 mg was used. Furthermore, the appetite score was significantly higher at 5 hours, suggesting a decreased appetite, and the amount of food consumed was about 16% lower [7].
BENEFITS OF PRESCRIBING LIRAGLUTIDE
GLP-1 RAs potentiate glucose-induced insulinotropic action. GLP-1 RAs, the levels of which are increased by food intake, bind to pancreatic β-cell receptors and promote insulin synthesis and secretion. Glucagon secretion from α cells is also inhibited proportionally to the glucose concentration, which is considered to be mediated by an increase in insulin or somatostatin secretion or by an inhibitory effect via the vagus nerve. In addition, GLP-1 RAs induce the proliferation and differentiation of pancreatic β-cells and increase the β cell mass by inhibiting apoptosis. In this way, GLP-1 RAs exert cardiovascular and renal protective effects, improving nonalcoholic fatty liver disease through mechanisms including weight loss, blood glucose control, blood pressure reduction, lipid improvement, insulin resistance improvement, and inflammation and oxidative stress reduction [8].
Liraglutide (Saxenda, Novo Nordisk Inc) is a GLP-1 RA used as an injection treatment for weight management. It was released as a blood glucose control treatment for patients with diabetes, but it was approved for use as an obesity treatment by the US Food and Drug Administration (FDA) in 2014, as it was found to be effective for weight loss without hypoglycemia in obese people who did not have diabetes. Administering liraglutide as a subcutaneous injection increases safety and delays absorption in the colon [3]. Once released into the bloodstream, 16-carbon fatty acid chains bind to albumin, preventing the breakdown of dipeptase-4. As a result, the half-life of GLP-1 RAs, which would otherwise be as short as 2 minutes, is extended to approximately 10 to 18 hours, enabling liraglutide to maintain adequate blood levels even when administered once a day.
The Satiety and Clinical Adiposity – Liraglutide Evidence (SCALE) Maintenance Study reported weight loss benefits of liraglutide [9]. In particular, when examining weight change when orlistat (Xenical, Cheplapharm) or liraglutide was injected in adults without diabetes who had a body mass index of 30 to 40 kg/m2, the weight loss effect was greater when liraglutide was used, especially when a high dose was used [10]. Liraglutide has a long-term effect of more than 3 years on weight loss in adults with prediabetes [11]. A meta-analysis reported a weight loss of 4.19 kg (4.16%), a decrease in body mass index of 1.55 kg/m2, and a decrease in waist circumference of 3.11 cm when liraglutide was used [12]. In addition, fasting blood glucose and hemoglobin A1c levels improved when liraglutide was administered to adults without diabetes. The liraglutide group also showed a lower incidence of prediabetes and diabetes than the control group [11,13]. Consistent results were also found for patients with diabetes [14].
In the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) study, the incidence of cardiovascular disease was lower when liraglutide was used in patients with type 2 diabetes [15]. Nonfatal myocardial infarction, stroke, and hospitalization for heart failure also showed reductions with liraglutide use, but without statistical significance. Various studies have found that, among patients with type 2 diabetes, a history of myocardial infarction or stroke, or arteriosclerotic cardiovascular disease, liraglutide use was associated with a lower incidence of cardiovascular disease than in the control group [16].
Other effects of liraglutide are well known. A meta-analysis reported reductions in systolic blood pressure, diastolic blood pressure, and low-density lipoprotein cholesterol levels with liraglutide [12]. A lower urine albumin/creatinine ratio has been reported with liraglutide (3.0 mg) in patients with type 2 diabetes [14]. These findings emphasize the positive effects of liraglutide on renal function [17]. However, caution is necessary in light of reports describing increased creatinine levels and acute renal failure due to dehydration caused by nausea, vomiting, and diarrhea, which are common side effects of liraglutide [18]. A significant improvement in fatty liver was observed after 48 weeks of liraglutide treatment [19]. In addition, the apnea-hypopnea index improved when obese adults with severe obstructive sleep apnea used liraglutide [20].
In a study involving adolescents aged 12 to 18 years with a body mass index of 30 kg/m2 or higher, those who used liraglutide (3.0 mg) for 56 weeks showed a significant weight loss of 3.2%, as compared to a weight gain of 2.2% in the control group. Twenty-six weeks after stopping treatment, both groups had gained weight, but compared to the initial period, the liraglutide use group had gained 1.5% and the control group had gained 4.6%, suggesting that liraglutide was effective for weight management, even in adolescents. Altogether, it was concluded that liraglutide has a substantial effect on weight loss in obese adolescents [21].
POINTS TO CONSIDER WHEN PRESCRIBING LIRAGLUTIDE
The side effects of liraglutide have been investigated [18]. The most common side effects are gastrointestinal, such as nausea, vomiting, indigestion, constipation, and diarrhea. These side effects are more common with higher doses of liraglutide, but they are usually temporary and rarely lead to treatment discontinuation. Hypoglycemia should be avoided when using insulin or sulfonylureas together with insulin-secreting agents. Blood glucose levels should be monitored, and the reduction of existing blood glucose-lowering drugs should be considered. Compensation for blood pressure reduction and stimulation of the sinus node and sympathetic nervous system appear to speed up the pulse. The discontinuation of liraglutide may be considered if the heart rate continues to increase.
Although uncommon, liraglutide has been shown to cause mild pancreatitis, with elevated serum amylase or lipase levels. If acute pancreatitis develops, liraglutide should be discontinued and readministered. It appears to affect gallbladder contractions by inhibiting cholecystokinin secretion. In the LEADER study, acute gallbladder or biliary tract disease increased when liraglutide was used, and a recent meta-analysis reported an increased risk of cholelithiasis. No significant increase in the risk of malignancy was observed. There was also no increase in the risk of pancreatic, breast, or prostate cancer. However, there are reports of medullary thyroid cancer in animal models; therefore, whether liraglutide increases the risk of this cancer in humans is unclear. Nonetheless, liraglutide should not be used in patients with a history or family history of medullary thyroid cancer, or in patients with type 2 multiple endocrine neoplasia.
Most side effects of liraglutide occur after its initiation or when the dose is rapidly increased. In addition, reactions (rash or itching) at the injection site, insomnia, dizziness, and fatigue may occur.
CONCLUSIONS
Liraglutide is an injectable formulation administered subcutaneously once daily, and its significant weight loss effect has been demonstrated in various clinical studies. In addition to the weight loss effect, it has been shown to improve various risk factors, such as blood pressure, dyslipidemia, and blood glucose levels, which are closely related to obesity. Clinical studies have not generally documented serious side effects that require discontinuation of liraglutide, but gastrointestinal side effects, such as nausea, vomiting, and digestive disorders, often occur. Nausea may continue to occur for a long time, potentially causing poor drug compliance. Although a clear causal relationship has not yet been proven, reports of liraglutide-associated cholelithiasis and pancreatitis warrant attention. Therefore, when prescribing liraglutide, a balanced discussion is required between patients and medical staff about the expected therapeutic and side effects of the drug.
Notes
Ethics statements
Not applicable.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
This work was supported by a National Research Foundation of Korea (NRF) grant, funded by the Ministry of Science and ICT of Korea (No. NRF-2021R1G1A1091471).
Author contributions
Conceptualization: JS, HSK; Data curation: all authors; Formal analysis: all authors; Funding acquisition: HSK; Investigation: HSK; Methodology: HSK; Project administration: HSK; Resources: HSK; Software: HSK; Supervision: HSK; Validation: HSK; Visualization: JS; Writing–original draft: JS; Writing–review & editing: all authors. All authors read and approved the final manuscript.