, Dong Il Shin, MD1, Sung Ho Her, MD2, Seung Hwan Han, MD3, Youngkeun Ahn, MD4, Dong-Soo Kim, MD5, Dong-Ju Choi, MD6, Hyuck Moon Kwon, MD7, Hyeon-Cheol Gwon, MD8, Seung-Woon Rha, MD9, Sang-Ho Jo, MD10, Sung Cil Lim, MD11, Jun-Pyo Myong, MD12, Sang Hong Baek, MD13
, Dong Il Shin, MD1, Sung Ho Her, MD2, Seung Hwan Han, MD3, Youngkeun Ahn, MD4, Dong-Soo Kim, MD5, Dong-Ju Choi, MD6, Hyuck Moon Kwon, MD7, Hyeon-Cheol Gwon, MD8, Seung-Woon Rha, MD9, Sang-Ho Jo, MD10, Sung Cil Lim, MD11, Jun-Pyo Myong, MD12, Sang Hong Baek, MD13 
1Department of Cardiovascular Medicine, Incheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Department of Cardiovascular Medicine, Daejeon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
3Department of Cardiovascular Medicine, Gil Medical Center, Gachon University, Incheon, Korea
4Department of Cardiovascular Medicine, Chonnam National University Hospital, Chonnam National University, Gwangju, Korea
5Department of Cardiovascular Medicine, Busan Paik Hospital, Inje University, Busan, Korea
6Department of Cardiovascular Medicine, Bundang Hospital, Seoul National University, Seongnam, Korea
7Department of Cardiovascular Medicine, Gangnam Severance Hospital, Yonsei University, Seoul, Korea
8Department of Cardiovascular Medicine, Samsung Medical Center, Sungkyunkwan University, Seoul, Korea
9Department of Cardiovascular Medicine, Guro Hospital, Korea University, Seoul, Korea
10Department of Cardiovascular Medicine, Pyeongchon Sacred Heart Hospital, Hallym University, Anyang, Korea
11Department of Cardiovascular Medicine, College of Pharmacy, The Catholic University of Korea, Bucheon, Korea
12Department of Occupational and Environmental Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
13Department of Cardiovascular Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
Copyright © 2019. Korean Society of Cardiovascular Disease Prevention; International Society of Cardiovascular Pharmacotherapy, Korea Chapter.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Conflict of Interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: Shin DI, Baek SH; Data curation: Shin DI, Kim DS, Choi DJ; Formal analysis: Her SH, Myong JP; Investigation: Han SH, Rha SW, Jo SH; Methodology: Lim SC; Resources: Ahn Y, Kwon HM; Supervision: Ahn Y, Gwon HC; Writing - original draft: Lee KY; Writing - review & editing: Lee KY, Baek SH.
Values are presented as means±standard deviation or number (%). Aspirin denotes 100 mg/day aspirin.
ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; BMI = body mass index; CCB = calcium channel blocker; COPD = chronic obstructive pulmonary disease; HDL-C = high density lipoprotein cholesterol; LDL-C = low density lipoprotein cholesterol; LVEF = left ventricle ejection fraction; SMD = standardized mean difference. TC = total cholesterol.
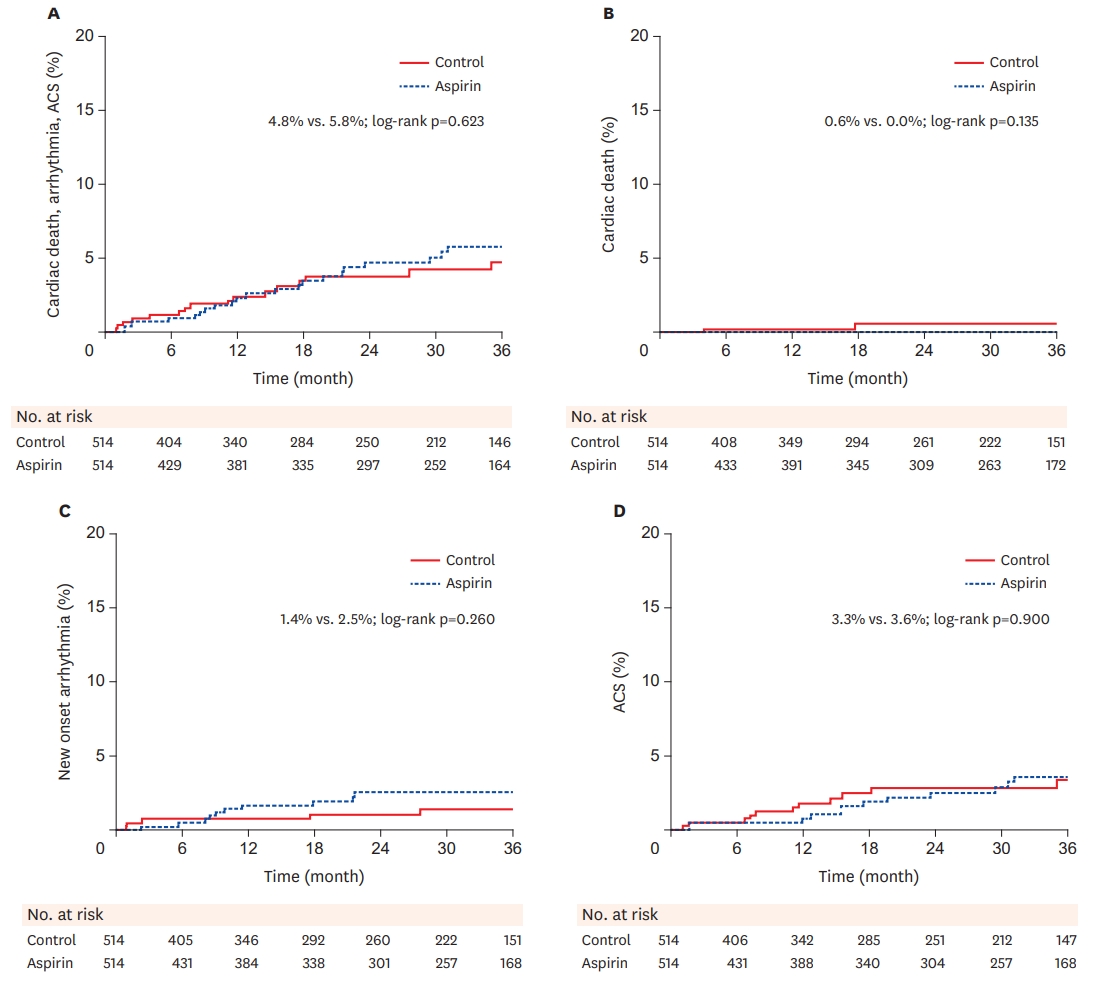
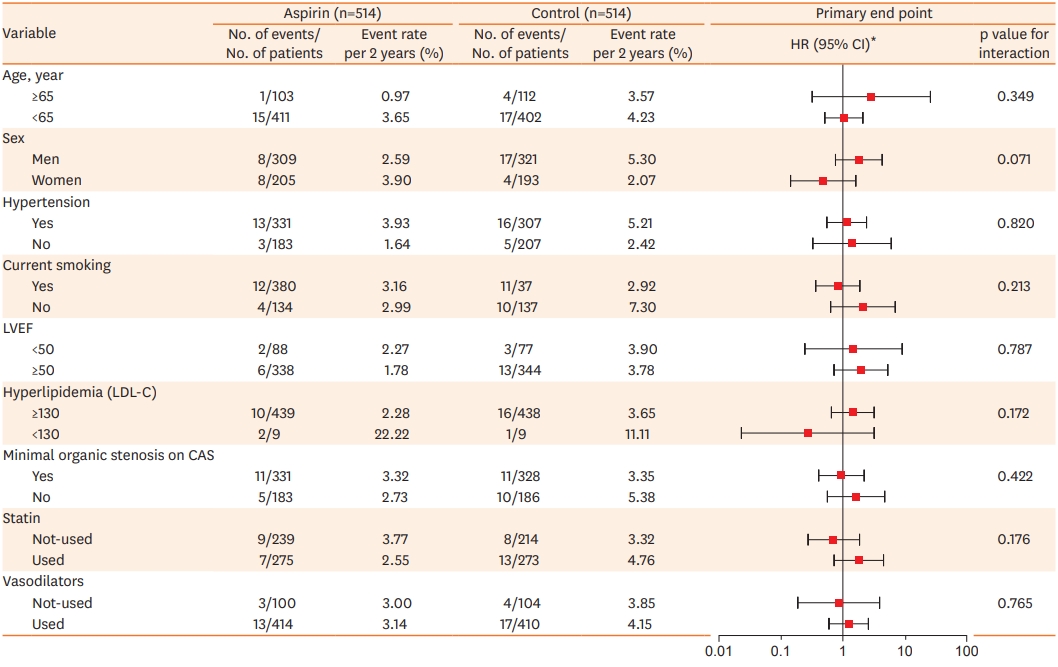
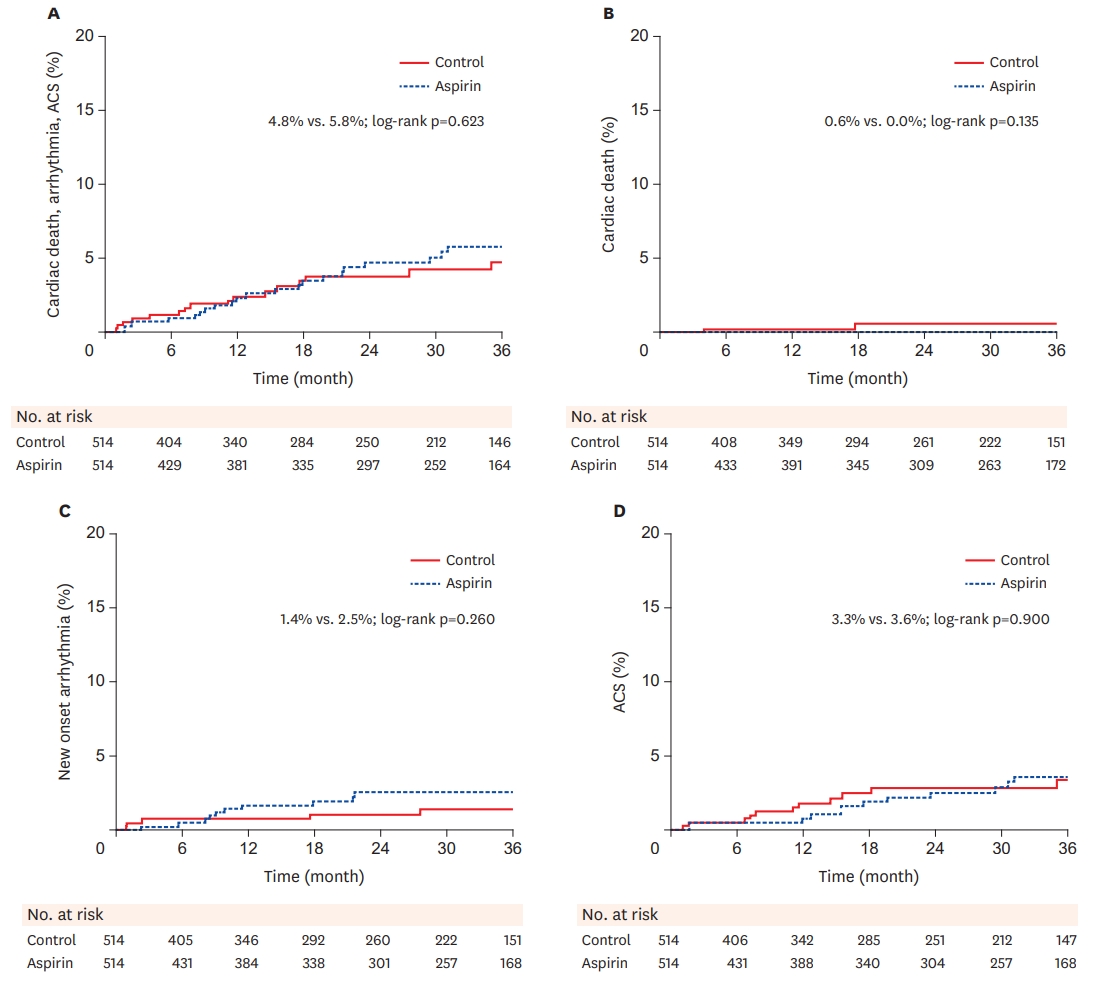
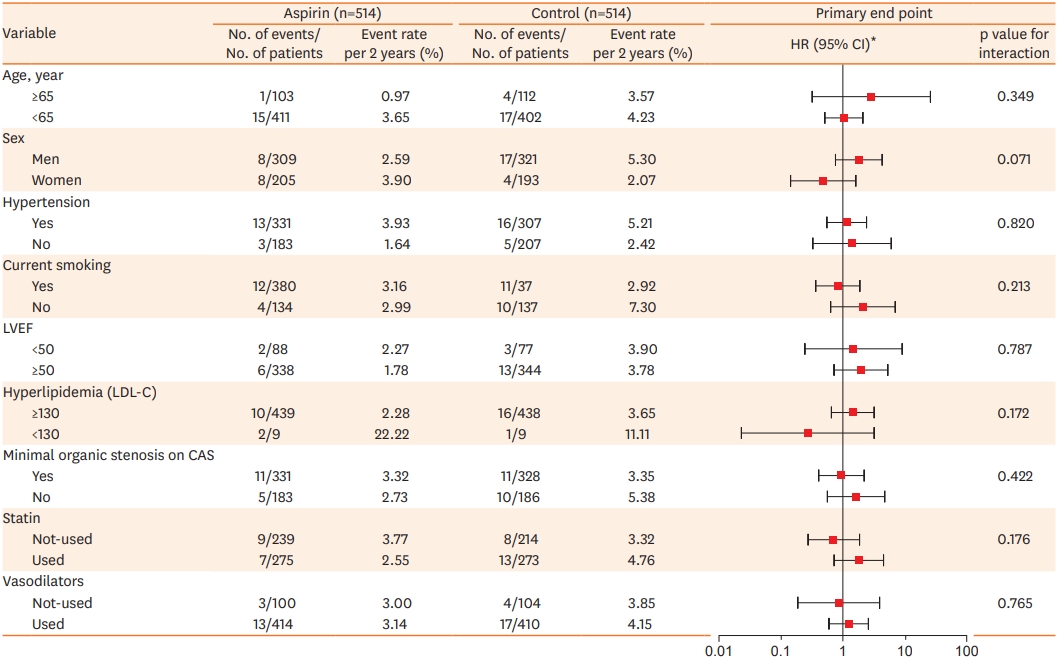
Values are presented as number (%). HRs are for the aspirin group as compared to the control group.
ACS = acute coronary syndrome; AV = atrioventricular; CD = cardiac death; CI = confidence interval; ED = emergency department; HR = hazard ratio; MACE = major adverse cardiac event; NSTEMI = non-ST elevation myocardial infarction; STEMI = ST elevation myocardial infarction; VA = vasospastic angina; VF = ventricular fibrillation; VT = ventricular tachycardia.
| Characteristics |
Present cohort |
Ishii et al.21) |
Lim et al.14) |
||||
|---|---|---|---|---|---|---|---|
| No aspirin (n=514) | Aspirin (n=514) | No aspirin (n=112) | Aspirin (n=112) | No aspirin (n=287) | Aspirin (n=434) | ||
| Enrollment | 2010–2015 | 1991–2010 | 2003–2014 | ||||
| Registry information | 11 multi-centers, prospective | Single center, retrospective | Single center, retrospective | ||||
| Race | Korean | Japanese | Korean | ||||
| Follow duration (yr) | 2.00 (0.86–3.01) | 5 | 4.34 | ||||
| Provocation drug | Ergonovine | Acetylcholine | Ergonovine | ||||
| Age (yr) | 55.94±10.75 | 55.55±10.93 | 67.0±8.4 | 66.0±9.5 | 55.0 (49.0–62.5) | 56.0 (49.0–62.0) | |
| Male | 309 (60.1) | 321 (62.5) | 65 (58.0) | 65 (58.0) | 243 (84.7) | 359 (82.7) | |
| Hypertension | 183 (35.6) | 207 (40.3) | 57 (50.9) | 52 (46.4) | 104 (36.2) | 156 (36.0) | |
| Diabetes mellitus | 43 (8.4) | 49 (9.5) | 27 (24.1) | 26 (23.2) | 66 (23.0) | 98 (22.6) | |
| Current Smoking | 134 (26.1) | 137 (26.7) | 52 (46.4) | 59 (52.7) | 87 (30.3) | 127 (29.3) | |
| Dyslipidemia | 93 (18.1) | 75 (14.6) | 60 (53.6) | 62 (55.4) | 62 (21.6) | 91 (21.0) | |
| BMI (kg/m2) | 24.62±3.15 | 24.82±3.02 | 23.7 ± 3.9 | 24.0 ± 3.1 | 24.7 (22.7–26.3) | 24.4 (22.8–26.0) | |
| Laboratory findings | |||||||
| Total cholesterol (mg/dL) | 176.29±37.31 | 173.38±35.66 | 190.3±34.2 | 188.8±31.7 | 171 (150–193) | 169 (150–197) | |
| Triglyceride (mg/dL) | 142.01±88.10 | 140.99±108.51 | 121.8±64.0 | 133.0±76.2 | 129 (88–191) | 128 (91–196) | |
| LDL (ml/dL) | 104.55±32.20 | 103.95±30.65 | 111.5±30.7 | 110.9±27.7 | 106 (86–123) | 105 (86–128) | |
| HDL (mg/dL) | 46.76±12.50 | 47.29±13.93 | 54.4±16.3 | 51.3±16.9 | 46 (39–55) | 45 (39–53) | |
| LVEF (%) | 64.93±6.56 | 64.37±6.63 | - | - | 64.0 (60.0–68.0) | 65.0 (61.0–68.0) | |
| CAG findings | |||||||
| Minimal organic stenosis | 183 (35.6) | 186 (36.2) | - | - | 86 (30.0) | 143 (32.9) | |
| Medication at discharge | |||||||
| Vasodilators | 414 (80.5) | 410 (79.8) | 23 (19.7) | 27 (24.1) | 177 (61.7) | 267 (61.5) | |
| CCB | 470 (91.4) | 460 (89.5) | 101 (90.2) | 104 (92.9) | 275 (95.8) | 420 (96.9) | |
| Statin | 275 (53.5) | 273 (53.1) | 40 (35.7) | 38 (33.9) | 113 (39.4) | 182 (42.0) | |
| ACEI/ARB | 81 (15.8) | 89 (17.3) | 25 (22.3) | 33 (29.5) | 43 (15.0) | 69 (15.9) | |
| Beta blocker | 22 (4.3) | 26 (5.1) | 7 (6.3) | 6 (5.4) | 0 (0.0) | 1 (0.2) | |
| Clinical outcome | |||||||
| All-cause of death | 2 (0.4) | 1 (0.2) | - | - | 9 (2.8) | 10 (2.2) | |
| Cardiac death | 2 (0.4) | 0 (0.0) | 0 (0) | 2 (1.8) | 3 (0.9) | 4 (0.9) | |
| Arrhythmia | 5 (1.0) | 10 (1.9) | - | - | - | - | |
| Myocardial infarction | 1 (0.2) | 0 (0.0) | 0 (0) | 0 (0) | 2 (0.6) | 9 (2.0) | |
| Unstable angina | 10 (1.9) | 12 (2.3) | 6 (5.4) | 2 (1.8) | - | - | |
| Rehospitalization/ED visit | 69 (13.4) | 78 (15.2) | - | - | 36 (11.2) | 94 (20.6) | |
Values are presented as means±standard deviation or number (%). HRs are for the LAS group, as compared control group.
ACEI = angiotensin converting enzyme inhibitor; ARB = angiotensin receptor blocker; BMI = body mass index; CAG = coronary angiogram; CCB = calcium channel blocker; ED = emergency department; HDL = high density lipoprotein; HR = hazard ratio; LAS = lung allocation score; LDL = low density lipoprotein; LVEF = left ventricle ejection fraction; VA = vasospastic angina.

 PubReader
PubReader ePub Link
ePub Link Cite
Cite